🛍️ Products
❤️ Health
🌿 Wellness
💪 Performance
🤝 Relationships
🛍️ Products
❤️ Health
🌿 Wellness
💪 Performance
🤝 Relationships
Ejaculation is often understood simply as the expulsion of semen from the penis during sexual climax. However, beneath this seemingly straightforward event lies an intricate symphony of neurological signals, hormonal influences, and precisely coordinated muscular contractions. This article dives deep into the fascinating mechanics of ejaculation, breaking down the complex physiological process into understandable components.
According to research published in the Journal of Sexual Medicine, ejaculation consists of two distinct yet seamlessly integrated phases:
Let’s explore each phase in detail to understand the remarkable orchestration of biological events that occur.
The emission phase begins with sexual arousal and continues until just before the moment of ejaculation. During this phase, several key events occur simultaneously:
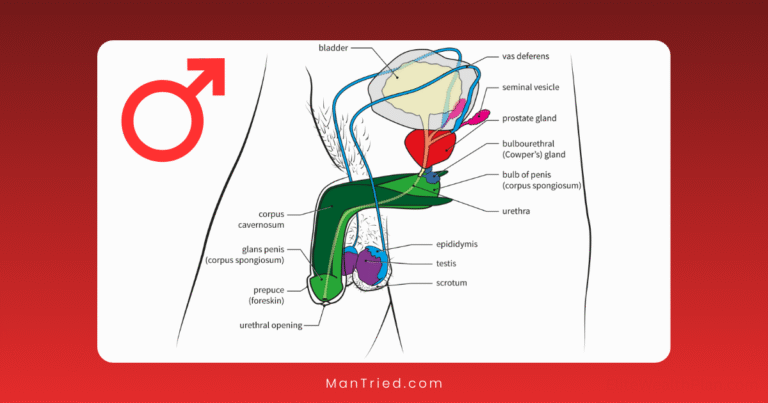
Stored in the epididymis (a coiled tube attached to each testicle), sperm cells are inactive until sexual arousal triggers their movement. According to Britannica Science, muscular contractions in the epididymis and vas deferens (sperm ducts) propel sperm toward the ampulla, a widened portion of the vas deferens near the prostate.
Multiple accessory glands activate to contribute their specialized fluids:
Research from the National Institutes of Health indicates that these secretions are produced in a specific sequence, creating a layered composition in the final ejaculate that optimizes sperm survival and function.
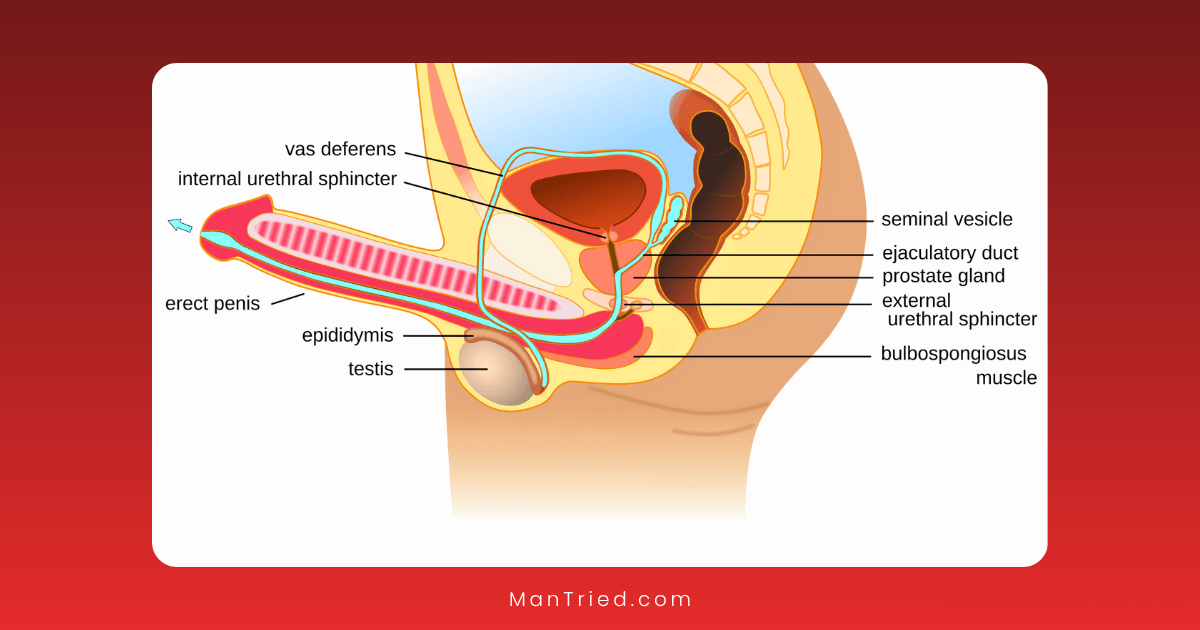
A critical event during emission is the closure of the bladder neck (internal sphincter). This prevents retrograde ejaculation—the backflow of semen into the bladder—and ensures forward propulsion of seminal fluid.
According to a 2023 study in European Urology, this process is controlled by alpha-adrenergic receptors responding to norepinephrine released from sympathetic nerve fibers.
The emission phase is primarily governed by the sympathetic nervous system—the same system responsible for our “fight or flight” response. Key neural components include:
Dr. Marcel Waldinger, a renowned researcher in sexual medicine, explains: “The sympathetic nervous system activation during emission explains why intense excitement or anxiety can sometimes trigger premature ejaculation—the system is already in a heightened state of arousal.”
Once emission is complete and seminal fluid has collected in the bulbar urethra, the expulsion phase begins. This phase represents what most people recognize as ejaculation—the forceful expulsion of semen from the penis.
The expulsion phase involves rhythmic contractions of several muscle groups:
Research from the American Physiological Society has measured the pressure generated during these contractions, finding that the average intra-urethral pressure during ejaculation can reach 200-500 cm H₂O—enough force to propel semen up to 30 centimeters in some cases.
During expulsion, the external urethral sphincter (a muscle that normally keeps the urethra closed) relaxes to allow the passage of semen. This relaxation is coordinated with the contraction of other muscles to ensure efficient expulsion.
Unlike emission, the expulsion phase involves a complex interplay between sympathetic, parasympathetic, and somatic nervous systems:
Recent research published in Nature Reviews Urology has identified specific lumbar spinothalamic (LSt) cells in the spinal ejaculation generator that are essential for coordinating ejaculation. These cells integrate sensory input from the genitals with descending signals from the brain to trigger the ejaculatory reflex at the appropriate time.
While ejaculation is primarily a spinal reflex, the brain plays crucial roles in both initiating and modulating the process:
Several brain regions are activated during ejaculation, as revealed by functional MRI studies published in The Journal of Sexual Medicine:
The timing and intensity of ejaculation are regulated by a delicate balance of neurotransmitters:
This neurochemical balance explains why certain medications, particularly selective serotonin reuptake inhibitors (SSRIs), can delay ejaculation—a side effect sometimes utilized in treating premature ejaculation.
The average ejaculate volume ranges from 2-5 milliliters, though this can vary based on factors like age, health status, and time since last ejaculation.
According to research from the World Health Organization, a typical ejaculate contains:
These components are not thoroughly mixed but rather layered in the ejaculate, with the first portion containing more prostatic fluid and the later portions containing more seminal vesicle fluid and sperm.
Following ejaculation, men enter a refractory period during which another ejaculation cannot occur. According to research published in the International Journal of Impotence Research, this period varies significantly between individuals:
The physiological basis for this refractory period involves several mechanisms:
Multiple factors can influence the ejaculatory process:
Understanding the physiological process of ejaculation provides insight into various dysfunctions:
Affecting approximately 30% of men at some point, premature ejaculation involves ejaculation that occurs sooner than desired. Research from the International Society for Sexual Medicine suggests it often results from hypersensitivity of the ejaculatory reflex or imbalances in serotonin signaling.
Characterized by significant delay or inability to achieve ejaculation despite adequate stimulation. According to the American Urological Association, this can result from neurological issues, hormonal imbalances, or psychological factors.
Occurs when semen enters the bladder rather than being expelled through the urethra, often due to dysfunction of the bladder neck closure mechanism. This is common after certain prostate surgeries or in men with diabetic neuropathy.
The complete absence of ejaculation despite orgasm (dry orgasm) or the inability to reach orgasm. This can result from nerve damage, certain medications, or psychological issues.
Recent advances in understanding ejaculation mechanics include:
Dr. Emmanuele Jannini, a leading researcher in sexual medicine, notes: “We’re moving toward a more nuanced understanding of ejaculation that recognizes it not as a simple reflex but as a complex process involving multiple systems and capable of significant plasticity and learning.”
Ejaculation represents one of the most complex and precisely coordinated physiological processes in the male body. From the careful preparation and collection of reproductive fluids to their forceful expulsion, the process involves intricate communication between the brain, spinal cord, autonomic nervous system, and multiple organ systems.
Understanding this remarkable process not only satisfies scientific curiosity but also provides the foundation for addressing the many issues that can affect this important aspect of male sexual function. As research continues to unravel the complexities of ejaculation, we can expect more effective treatments for ejaculatory dysfunctions and a deeper appreciation for this fundamental aspect of human reproduction.